Skin Hurts To Touch But No Rash | Reasons And Treatment. You reach for your shirt in the morning, and the fabric stings. Someone pats you on the shoulder and it feels like a sunburn. Your skin hurts to touch — but when you look in the mirror, there’s no rash, no redness, nothing. Also Read https://memedicine.org/what-are-progressive-lenses/
This confusing symptom is more common than most people realize. When skin is painful to touch but no visible cause exists, the problem usually lies not in the skin itself, but in how your nervous system is processing sensory signals. Understanding what’s happening — and why — is the first step toward effective relief.
This guide covers every major cause of touch-sensitive skin without a rash, how each condition is diagnosed, and what treatments actually work.
What Does It Mean When Your Skin Hurts to Touch But Has No Rash?
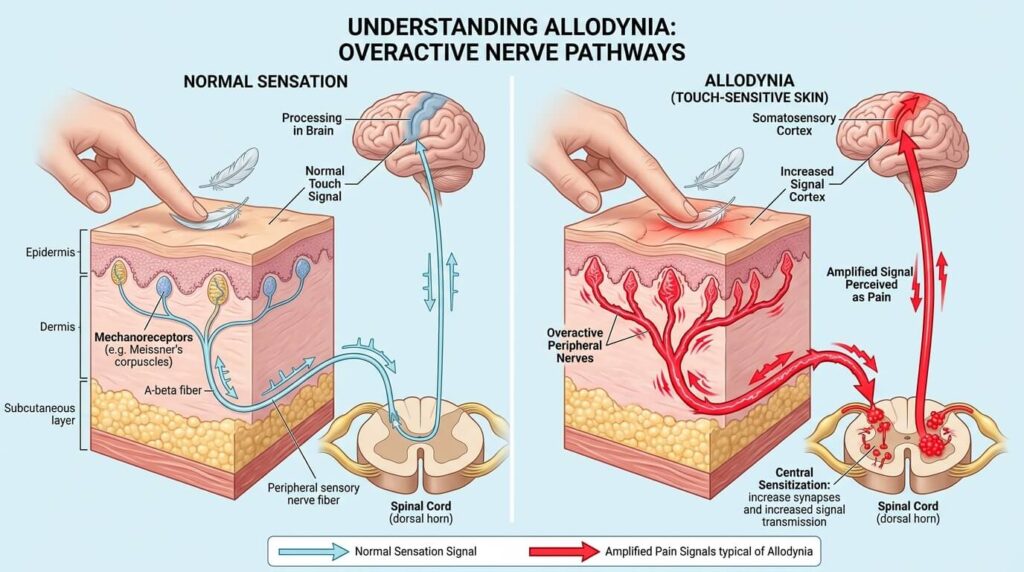
Skin pain without a visible rash is almost always a neurological symptom rather than a dermatological one. Your skin contains a vast network of sensory nerve fibers. When those fibers or the central nervous system pathways they connect to become disrupted or overly sensitive, they can fire pain signals in response to stimuli that should feel neutral — or even pleasant.
This phenomenon has a clinical name: allodynia (from the Greek allos meaning “other” and odyne meaning “pain”). It describes pain arising from a stimulus that does not normally cause pain, such as light touch, clothing, or mild temperature changes.
Allodynia is not a diagnosis in itself — it is a symptom of an underlying condition affecting the nervous system.
The 3 Types of Allodynia (Touch-Sensitive Skin Pain)
Understanding which type of allodynia you experience helps narrow down the cause:
| Type | Trigger | Example |
|---|---|---|
| Tactile (Static) Allodynia | Light touch or gentle pressure | Handshake, clothing contact |
| Mechanical (Dynamic) Allodynia | Something moving across the skin | Towel drying, a breeze |
| Thermal Allodynia | Mild temperature change | Cool air, lukewarm water |
Most people with allodynia experience more than one type simultaneously.
Common Causes of Skin Pain Without a Rash
1. Fibromyalgia
Fibromyalgia is one of the most frequent causes of widespread skin sensitivity without any visible skin changes. It is a chronic pain condition characterized by central sensitization — a state in which the brain and spinal cord amplify all pain signals, including those from touch.
People with fibromyalgia often describe their skin as feeling bruised, raw, or burned even when nothing is touching it. The sensitivity tends to shift across the body and may worsen with fatigue, stress, or weather changes.
Associated symptoms: Fatigue, sleep disturbances, cognitive difficulties (“fibro fog”), muscle aches, and heightened sensitivity to light and sound.
2. Migraine and Migraine-Associated Allodynia
Research indicates that roughly 50% of people with chronic migraine develop allodynia, especially as migraines become more frequent. During and after a migraine attack, the nervous system becomes so sensitized that the scalp, face, neck, and even arms can become extremely painful to touch.
This is why many migraine sufferers cannot wear glasses, earrings, or tight clothing during an attack — the contact is genuinely painful.
Key fact: Allodynia during migraine is a sign of central sensitization and may indicate that the migraine is progressing. Treating a migraine early, before allodynia sets in, is significantly more effective.
3. Peripheral Neuropathy
Peripheral neuropathy occurs when the nerves outside the brain and spinal cord are damaged or dysfunctional. These nerves carry sensory signals from the skin, so when they malfunction, they can produce burning, tingling, stabbing pain — or severe touch sensitivity.
Peripheral neuropathy can be caused by:
- Diabetes (diabetic neuropathy): One of the leading causes. Chronically high blood sugar damages small nerve fibers, often starting in the feet and hands.
- Vitamin deficiencies: Deficiencies in B12, B1 (thiamine), B6, and vitamin D are well-documented causes of neuropathic pain.
- Autoimmune diseases: Lupus, rheumatoid arthritis, and Sjögren’s syndrome can attack peripheral nerves.
- Alcohol use disorder: Chronic alcohol use is directly toxic to nerve tissue.
- Medications: Chemotherapy drugs (chemotherapy-induced peripheral neuropathy, or CIPN), certain antibiotics like metronidazole, and HIV medications can all damage peripheral nerves.
- Infections: Lyme disease, shingles (even before the rash appears), and HIV can cause neuropathic skin pain.
4. Postherpetic Neuralgia (Shingles Nerve Pain)
The varicella-zoster virus that causes chickenpox lies dormant in nerve tissue for decades. When it reactivates as shingles, it inflames the nerve fibers along a specific dermatomal path (a strip of skin supplied by one nerve root). After the rash resolves, the nerve damage left behind can cause months or years of severe burning and touch sensitivity — a condition called postherpetic neuralgia (PHN).
Importantly, skin pain often begins one to five days before the shingles rash appears, meaning many people experience painful skin with no visible cause during this prodromal phase.

5. Multiple Sclerosis (MS)
Multiple sclerosis damages the myelin sheath surrounding nerve fibers in the central nervous system. This disrupts signal transmission and can produce a wide variety of sensory abnormalities, including allodynia, burning skin pain (known as MS-related dysesthesia), and the sensation of tight banding around the torso (“MS hug”).
6. Complex Regional Pain Syndrome (CRPS)
CRPS is a chronic pain condition that usually develops after an injury to a limb — sometimes a minor one like a sprain or fracture. The nervous system goes into an abnormal state of sustained pain amplification, causing severe allodynia, burning pain, swelling, and changes in skin color or temperature in the affected area.
7. Lupus and Autoimmune Conditions
Systemic lupus erythematosus (SLE) and other autoimmune diseases can cause nerve inflammation that manifests as skin hypersensitivity. The pain may precede other symptoms and can fluctuate with disease activity.
8. Anxiety, Depression, and Psychological Stress
Chronic psychological stress and anxiety activate the body’s stress-response systems, which directly influence pain processing. Elevated cortisol and neuroinflammatory changes can lower the pain threshold, making skin more sensitive to touch.
Depression is also associated with increased pain sensitivity. Importantly, this is a physiological mechanism — not “imaginary” pain. The brain changes associated with chronic stress are real and measurable.
9. Restless Legs Syndrome (RLS) and Small Fiber Neuropathy
Small fiber neuropathy — damage specifically to the smallest sensory nerve fibers — frequently causes burning, tingling, or painful sensitivity across the skin without any visible abnormality. It is commonly missed because standard nerve conduction studies often return normal results; a skin biopsy measuring intraepidermal nerve fiber density is required for diagnosis.
10. COVID-19 and Post-COVID Syndrome (Long COVID)
Emerging data suggest that SARS-CoV-2 infection can cause peripheral nerve damage, likely through inflammation and microvascular injury. Skin pain, burning, and allodynia have been reported both during acute COVID-19 and as part of long COVID, sometimes persisting for months.
11. Sunburn Without Visible Redness (Phototoxic Reactions)
Mild phototoxic or photosensitive reactions, or early UV damage before redness appears, can cause the skin to feel painfully sensitive to touch. This is one of the few causes where the problem is genuinely in the skin rather than the nervous system — though it typically resolves within days.
12. Hormonal Changes
Hormonal fluctuations — particularly estrogen changes during menstruation, pregnancy, perimenopause, or thyroid dysfunction — can affect pain sensitivity. Some women report significant skin hypersensitivity in the days before menstruation (premenstrual allodynia).
Symptoms That Accompany Skin Pain Without a Rash
The character of the pain and any accompanying symptoms help identify the underlying cause:
Pain descriptions commonly reported:
- Burning or stinging sensation
- Raw or sunburned feeling
- Electric shock-like jolts
- Throbbing or deep aching
- Itching that transitions to pain
Red flag symptoms requiring urgent evaluation:
- Sudden onset of severe skin pain with no known cause
- Skin pain accompanied by fever, confusion, or weakness
- Rapidly spreading pain
- Pain with numbness or paralysis
- Skin pain following trauma or injury
How Is Touch-Sensitive Skin Without a Rash Diagnosed?
Diagnosis begins with a thorough history and physical examination. Your doctor will ask you to describe the quality, location, timing, and triggers of the pain — detail that is critical for distinguishing neuropathic pain from other types.
Self-assessment: You can perform a preliminary check by lightly brushing a dry cotton pad across the affected skin and applying a warm or cool compress. Pain in response to either stimulus suggests allodynic sensitivity, though a formal diagnosis requires a healthcare provider.

Diagnostic tests your doctor may order:
- Blood tests: Complete blood count, metabolic panel, HbA1c (for diabetes), B12 and vitamin D levels, thyroid function, inflammatory markers (ESR, CRP, ANA for autoimmune diseases)
- Nerve conduction studies (NCS) and electromyography (EMG): Assess large nerve fiber function
- Skin punch biopsy: The gold standard for diagnosing small fiber neuropathy; measures nerve fiber density in the skin
- MRI: Evaluates the brain and spinal cord for MS lesions, tumors, or structural issues
- Quantitative sensory testing (QST): Measures sensory thresholds objectively
Treatment Options for Skin That Hurts to Touch
Because allodynia is a symptom rather than a standalone condition, treatment targets the underlying cause. However, several approaches reduce the pain itself while the underlying issue is addressed.
Medications
Anticonvulsants (neuropathic pain agents):
- Pregabalin (Lyrica) and gabapentin are commonly prescribed for fibromyalgia, diabetic neuropathy, and postherpetic neuralgia. They reduce abnormal nerve firing.
Antidepressants:
- Serotonin-norepinephrine reuptake inhibitors (SNRIs) like duloxetine (Cymbalta) and venlafaxine reduce central pain sensitization. Tricyclic antidepressants (e.g., amitriptyline) are also effective for neuropathic pain.
Topical treatments:
- Lidocaine patches or cream provide localized numbing by blocking sodium channels in nerve endings.
- Capsaicin cream (derived from chili peppers) depletes substance P in nerve terminals, reducing pain signal transmission over time. Initially causes burning; this diminishes with repeated use.
- Menthol-based creams provide temporary cooling relief for thermal allodynia.
Migraine-specific treatments:
- Triptans (sumatriptan, rizatriptan) are most effective when taken early, before allodynia develops. Once allodynia is present, triptans become significantly less effective — a critical reason for early migraine treatment.
- CGRP antagonists (newer migraine-prevention medications) have shown benefit for migraine-associated allodynia.
Anti-inflammatory medications:
- NSAIDs may help in cases where inflammation is contributing to nerve irritation.
Physical and Interventional Therapies
Desensitization therapy: A structured physical therapy approach where a therapist gradually exposes the skin to increasingly intense stimuli over many sessions. The nervous system recalibrates its response threshold over time. Particularly effective for CRPS and post-injury allodynia.
Nerve blocks: Injections of local anesthetic (sometimes combined with corticosteroids) around specific nerves or nerve clusters can interrupt pain signaling. Useful for localized neuropathic pain.
Transcutaneous electrical nerve stimulation (TENS): Low-voltage electrical current applied to the skin can disrupt pain signals sent to the brain.
Spinal cord stimulation (SCS): A surgically implanted device delivers low-level electrical impulses directly to the spinal cord, effectively overriding or suppressing pain signals. Reserved for severe, treatment-resistant cases.
Botulinum toxin (Botox) injections: Has shown benefit in some cases of CRPS and migraine-related allodynia.
Psychological and Lifestyle Approaches
Cognitive behavioral therapy (CBT): Helps patients change their relationship with pain, reduce catastrophizing, and develop coping strategies. Has strong evidence for chronic pain conditions including fibromyalgia.
Mindfulness-based stress reduction (MBSR): Mindfulness practice reduces activity in pain-processing brain regions and decreases central sensitization.
Regular low-impact exercise: Exercise is one of the most consistently evidence-supported interventions for chronic pain. It reduces neuroinflammation, improves sleep, and raises pain thresholds. Swimming, walking, and yoga are particularly accessible.
Sleep optimization: Poor sleep dramatically amplifies pain sensitivity. Addressing insomnia — through sleep hygiene, CBT-I (cognitive behavioral therapy for insomnia), or medication when appropriate — can meaningfully reduce allodynia.
Dietary considerations: Anti-inflammatory diets (rich in omega-3 fatty acids, fruits, vegetables, and whole grains) may reduce neuroinflammation. For diabetic neuropathy, tight glycemic control is the single most important intervention.
Stress management: Since psychological stress directly lowers the pain threshold, reducing stress through any effective means — therapy, exercise, social connection, relaxation techniques — has a real physiological impact on pain.
Addressing Deficiencies
If blood tests reveal vitamin B12 or vitamin D deficiency, supplementation can produce significant improvement in neuropathic pain symptoms over several weeks to months.
Comparison: Key Conditions Causing Skin Pain Without a Rash
| Condition | Pain Character | Other Key Features | Primary Treatment |
|---|---|---|---|
| Fibromyalgia | Widespread, shifting, burning | Fatigue, sleep issues, fibro fog | Duloxetine, pregabalin, exercise |
| Migraine allodynia | Scalp/face/neck during attack | Headache, light/sound sensitivity | Triptans early, CGRP antagonists |
| Diabetic neuropathy | Feet/hands, burning, tingling | History of diabetes, numbness | Glycemic control, gabapentin |
| Postherpetic neuralgia | Unilateral band, severe burning | Prior shingles history | Lidocaine patches, capsaicin, TCA |
| MS dysesthesia | Variable, electric shock quality | Visual changes, weakness, fatigue | MS disease-modifying therapy |
| CRPS | Limb-localized, severe | Swelling, skin color changes | Desensitization PT, nerve blocks |
| Small fiber neuropathy | Burning feet/hands | Normal NCS | Skin biopsy diagnosis; treat cause |
| Vitamin deficiency | Diffuse, tingling | Dietary history, fatigue | Targeted supplementation |
When to See a Doctor
See a doctor promptly if:
- Skin pain is interfering with daily activities or sleep
- The pain started suddenly or is worsening rapidly
- You have other neurological symptoms such as numbness, weakness, or vision changes
- Pain is accompanied by fever, unintentional weight loss, or fatigue
- You have a known condition like diabetes or MS and notice new skin sensitivity
- Over-the-counter pain relievers are not helping
Seek emergency care if skin pain is severe, starts suddenly after trauma, or is accompanied by confusion, paralysis, or chest pain.
Can Touch-Sensitive Skin Be Prevented?
Full prevention is not always possible, but certain steps reduce the risk:
- Control diabetes diligently: Tight blood sugar management is the most powerful way to prevent diabetic neuropathy.
- Get the shingles vaccine (Shingrix): Highly effective at preventing shingles and significantly reduces the risk of postherpetic neuralgia.
- Address vitamin deficiencies early: Routine blood work can catch B12 and D deficiencies before nerve damage occurs.
- Treat migraines early and consistently: Early triptan use prevents the central sensitization that leads to allodynia.
- Maintain a healthy lifestyle: Regular exercise, a balanced diet, adequate sleep, and stress management all reduce the risk of conditions that cause neuropathic pain.
- Limit alcohol: Chronic heavy drinking is directly neurotoxic.
- Know your family history: If fibromyalgia, MS, lupus, or diabetes run in your family, proactive monitoring is worthwhile.
Living With Skin Sensitivity: Practical Tips
Managing day-to-day life when skin hurts to touch requires practical adaptations alongside medical treatment:
- Choose clothing carefully: Loose-fitting garments in soft natural fabrics (cotton, bamboo, modal) minimize mechanical stimulation. Avoid seams over sensitive areas.
- Use lukewarm water: Avoid extreme temperatures in the shower. Test water with your elbow before stepping in.
- Communicate with those around you: Explain the condition to family, friends, and coworkers so they understand why certain touches or hugs are difficult.
- Track your triggers: Keep a pain diary noting what worsens or relieves symptoms. Patterns help guide treatment.
- Seek peer support: Fibromyalgia and neuropathy support communities — in person or online — offer practical coping strategies and emotional validation.

FAQ: Skin Hurts to Touch But No Rash
Q: What is it called when skin hurts to touch for no reason?
A: This is most often called allodynia — pain produced by stimuli that would not normally cause pain. It is a neurological symptom, not a skin condition, and it always has an underlying cause even when none is immediately obvious.
Q: Can anxiety cause skin to hurt when touched?
A: Yes. Chronic anxiety triggers physiological changes in the nervous system — including elevated neuroinflammatory markers and altered pain processing — that can genuinely lower the pain threshold and cause or worsen skin hypersensitivity.
Q: Why does my skin hurt to touch but there’s no bruise or rash?
A: Pain without visible skin changes indicates the problem originates in the nerve fibers or central nervous system rather than the skin tissue itself. Common causes include fibromyalgia, peripheral neuropathy, migraine-associated allodynia, vitamin deficiencies, and MS.
Q: Can fibromyalgia cause skin pain without a rash?
A: Yes, this is one of the hallmark features of fibromyalgia. Central sensitization causes the entire nervous system to amplify pain signals, often making even light clothing contact feel intensely painful.
Q: Is touch-sensitive skin a symptom of COVID or long COVID?
A: Emerging evidence suggests that SARS-CoV-2 can damage peripheral nerves through inflammation and microvascular injury. Burning skin pain and allodynia have been documented in both acute COVID-19 and long COVID.
Q: Can a vitamin deficiency make my skin sensitive to touch?
A: Yes. Deficiencies in vitamin B12 and vitamin D are well-established causes of peripheral neuropathy, which can present as burning, tingling, or allodynic skin pain. Blood testing can confirm deficiency, and supplementation often improves symptoms.
Q: How do I know if my skin sensitivity is from a migraine?
A: If skin pain (especially scalp, face, or neck) develops during or shortly after the onset of a headache, and resolves as the migraine resolves, migraine-associated allodynia is likely. Up to half of chronic migraine sufferers develop this pattern.
Q: What does neuropathic skin pain feel like?
A: People most commonly describe it as burning, electric, or stinging. It may feel like a severe sunburn, pins and needles, or sharp jolts. The defining characteristic is that it occurs in response to stimuli — like touch or temperature changes — that would not normally cause pain.
Q: Can skin pain without a rash go away on its own?
A: It depends on the cause. Allodynia associated with migraines often resolves between attacks. Allodynia from treatable causes like vitamin deficiency or shingles may improve significantly with treatment. Allodynia from chronic conditions like fibromyalgia or MS is typically managed rather than cured, though symptoms can fluctuate and improve.
Q: What is the first-line treatment for allodynia?
A: There is no single first-line treatment because allodynia is a symptom of many different conditions. The most effective approach is identifying and treating the underlying cause. For symptomatic relief, gabapentin, pregabalin, SNRIs, and topical lidocaine are among the most evidence-supported options.
Q: Can children have allodynia?
A: Yes. Allodynia can occur in children, most commonly in association with migraines or amplified musculoskeletal pain syndrome (AMPS) — a pediatric pain condition involving central sensitization.
Q: Is allodynia rare?
A: Allodynia itself is not rare — estimates suggest it affects between 7% and 10% of the general population. Among people with neuropathic pain conditions, it is even more common, affecting up to 50% of chronic migraine patients.
Q: Is there a connection between allodynia and autoimmune disease?
A: Yes. Several autoimmune conditions including lupus, Sjögren’s syndrome, and rheumatoid arthritis can cause or contribute to peripheral neuropathy and allodynia through nerve inflammation or autoantibody-mediated nerve damage.
Q: Can hormonal changes cause skin sensitivity?
A: Yes. Estrogen fluctuations during the menstrual cycle, pregnancy, and perimenopause can affect pain processing. Some women experience significantly heightened skin sensitivity in the premenstrual phase, sometimes called premenstrual allodynia.
Q: When should I go to the ER for skin pain?
A: Seek emergency care if skin pain is sudden and severe, follows physical trauma, is accompanied by fever and blistering (which may indicate early shingles), or is associated with neurological symptoms like muscle weakness, confusion, or loss of bladder control.
